
Mindy M. Horrow, MD,FACR, FSRU
Director of Body Imaging AEMC
Professor of Radiology
TJU Medical School
January, 2012
CTUrography
Technique
No oral contrast
Low dose non contrast of kidneys through bladder
125 cc IV contrast, image kidneys duringnephrographic phase (100-110 sec)
300 cc IV fluid, 6-8 minutes, roll patient 360
Re-scout
Image kidneys through bladder with 2D and 3Dreconstructions, zoom and view at wide windowsettings
Report
Full description of kidneys, including renal lengths,comment on contour, symmetry of collecting systems,displacement, etc.
Function (symmetry of nephrograms and pyelograms)
Comment about degree of collecting system, ureteral andbladder opacification, search carefully for filling defectsand irregularities
Other findings


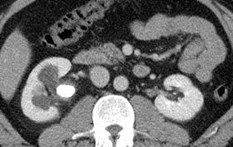
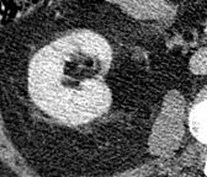
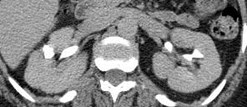
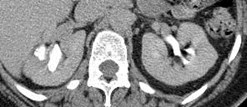
Normal Medullary Blush

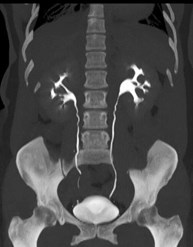
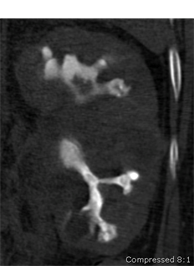
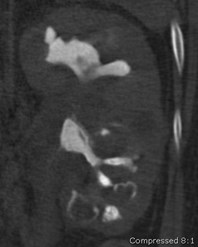
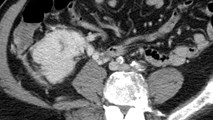
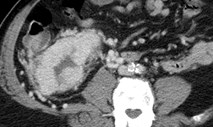
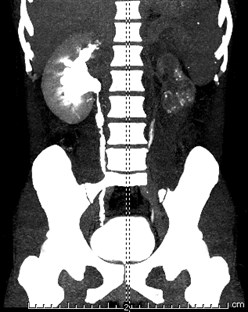
Delayed right nephrogram



Delayed right pyelogramwith perinephric fluid
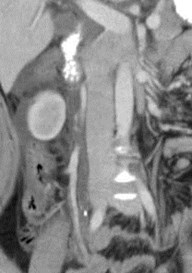

Acute high grade ureteral obstruction withforniceal rupture, secondary to calculus


Moderate caliectasis, minimalfunctional obstruction



Minimal dilatation secondaryto crossing vessel


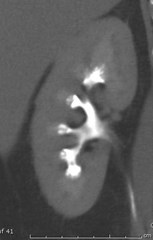

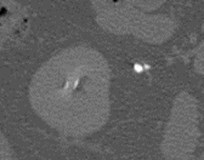
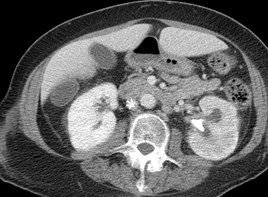
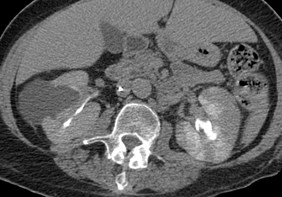
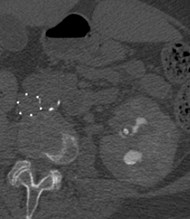
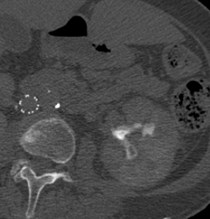
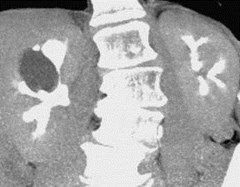
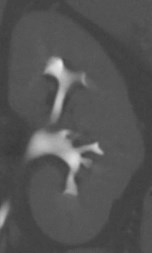
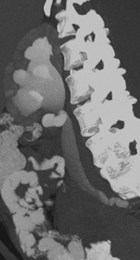
Medullary Sponge Kidney
Definition: Cystic dilatation of collecting tubules
0.5% incidence on IVU
Etiology: unknown
Range of findings from mild dilatation tubules in102 pyramids (renal tubular ectasia) thoughworsening dilatation to gross deformity ofcalyces with cysts and cyst like cavitiesextending through pyramids
Typical rounded and linear calcifications



Medullary Sponge Kidney
Normal Retrograde Urogram

Papillary Necrosis
Ischemia and necrosis in medullary portion of kidneyleads to inability to concentrate urine and polyuria,and decreased GFR
Sloughed papilla can lead to infection and obstruction
Two Types
–Medullary: intact fornices, discreet necrotic areas inpapillae
–Papillary: calyceal fornices and entire papillary surfacedestroyed leading to dilated, blunted calyces
Papillary Necrosis
Pyelonephritis
Obstruction
Sickle Cell Disease
Tuberculosis
Cirrhosis
Analgesics
Renal vein thombosis, renal tx rejection, radiation
Diabetes, dehydration
Systemic vasculitis

Papillary Necrosis with cortical scarring
Abnormally shaped, clubbed calyx
Sloughed papilla from papillary necrosis
Another example of papillarynecrosis with sloughed papillae


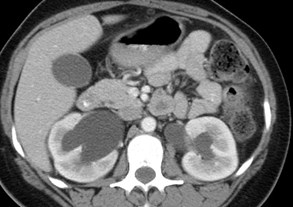
Large simple cyst causingsmooth impression on calyces



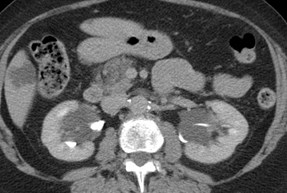

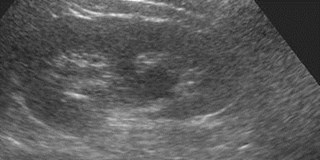
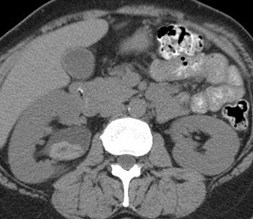
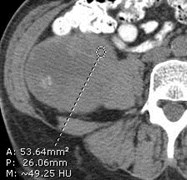
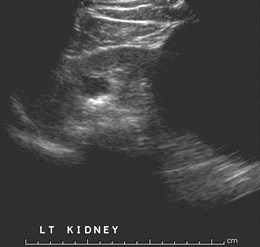
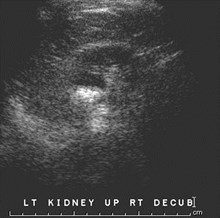
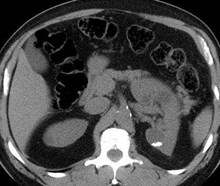
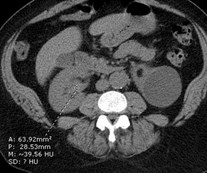
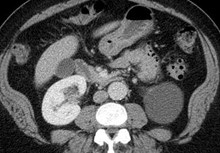
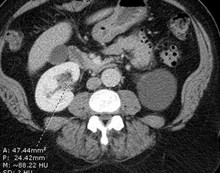
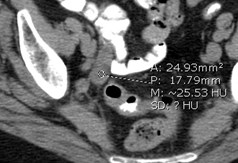
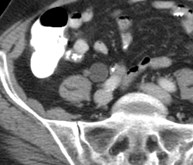
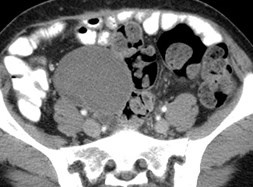
Parapelvic Cysts, Accessory Calyx
Parapelvic Cysts
Not true renal cysts, may be lymphatic in origin ordevelop from embryologic rests
Typically asymptomatic, but can be associated withhypertension, hematuria or hydronephrosis
May be difficult to distinguish from hydronephrosisor dilated renal pelvis on ultrasound or non-contrastCT


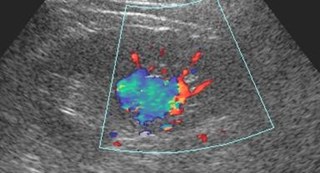
Renal Varix



Oncocytoma
Oncocytomas
Benign tumors, no metastatic potential
Most common in middle to older agedmen
Homogeneous enhancement on CT
Pseudocapsule, central scar in biggerlesions
“Spoke wheel” arteriographic pattern




Renal Cell Carcinoma
Hemorrhage and Amputated calyx


Calyceal Diverticulum
Urine containing cavity in renal parenchymacommunicating with collecting system throughnarrow channel
Two types
–Related to minor calyx in upper pole
–Communicates with renal pelvis or major central calyx
Usually asymptomatic, occasionally pain, UTI
Mobile calculi or milk of calcium are characteristic
US: simple cyst or cyst with calcification
BJ Radiology 2001;74:595

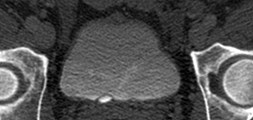

38 year old
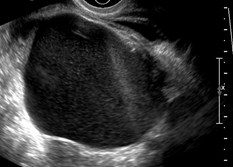
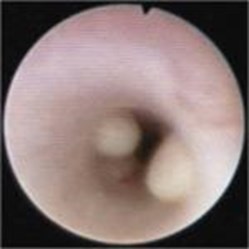
SimpleUreterocele
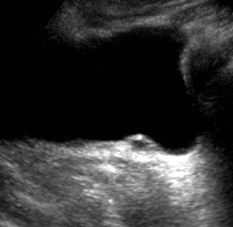
Ultrasound appearance ofsimple ureterocele


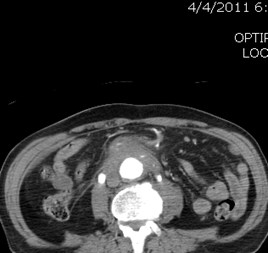
Routine positive stone search study
Simple ureterocele only visualized with CTU

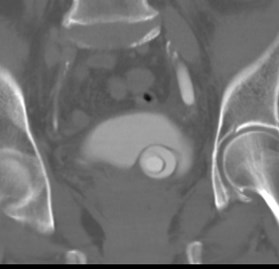
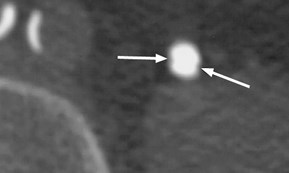
Simple ureterocele with calculus
Simple Ureterocele with calculus
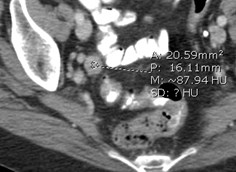
Prolapse of mucosa of terminal segment of ureter throughureterovesical orifice into bladder
Hyperplastic response to some degree of meatalobstruction
Since there is no muscle support of double mucosal wallsof prolapsed segment, it dilates, fills with urine andprotrudes into bladder
Simple ureterocele: normal position ureteral orifice,obstruction can be congenital or acquired secondary toinflammation
Ectopic ureterocele: protrusion of dilated submucosalportion of ectopic ureter, associated with duplicatedcollecting systems, from the upper pole moiety, insertsinferior to normal orifice
Radiographics 2002;22:1139




Pseudoureterocele
Cobra-head shaped distal ureter withincomplete distal ureteral obstruction usuallydue to tumor or calculus.
Lucency surrounding it is thicker than aureterocele and is poorly defined and possiblyirregular.
More likely than a ureterocele when there isasymmetry of dilated ureteral lumen,obstruction of upper tract and evidence of anacquired cause such as a calculus or abnormalvesical mucosal pattern
Radiology 2002;225:781

Papillary urothelial cell CA of renal pelvis
(originally interpreted as a blood clot in the renal pelvis)


Hematuria
Non con

Urothelial malignancy distal ureter


Bladder images from CT Urogram
Multifocal urothelial tumors
Patterns of UrothelialMalignancy in Renal Pelvis
Single or multiple irregular filling defects
Filling defects in dilated calyces
Calyceal amputation
Decreased or absent excretion withoutrenal enlargement secondary tolongstanding obstruction with atropy
Hydronephrosis with renal enlargement

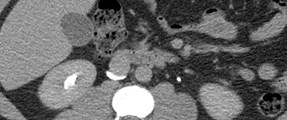
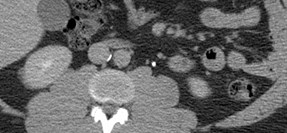
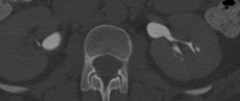
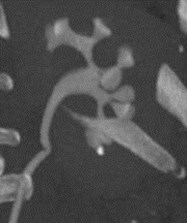
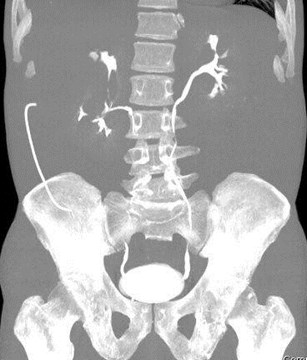
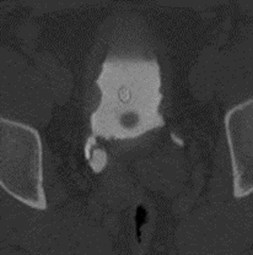
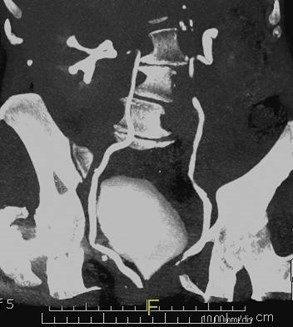
Circumcaval (Retrocaval)Ureter
Circumcaval Ureter
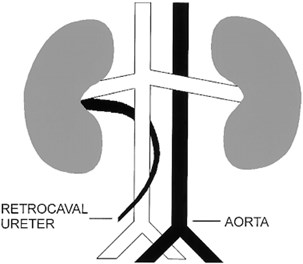
Circumcaval Ureter
IVC formed at 6-8 weeks as composite of 3paired sets of embryonic veins
Right supracardinal vein fails to form and rightposterior cardinal vein persists
Proximal right ureter passes posterior to IVC,emerges to right of aorta, eventually lyinganterior to right iliac vessels
May lead to obstruction and infections
Radiographics 2000;20:639

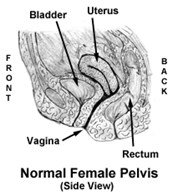
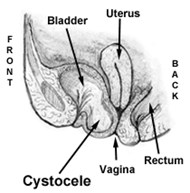
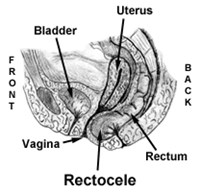
Grading of Cystoceles
1.Mild bladder descent into vagina
2. Bladder descends to vaginal orifice
3. Bladder protrudes through vagina

![MPj04001480000[1]](data/images/img106.jpg)
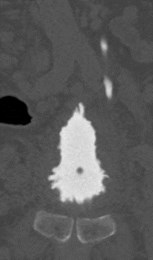
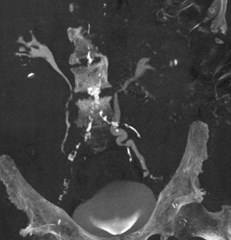
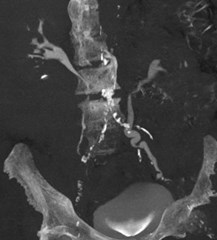
“Christmas Tree” Bladder
Thickened wall
Pear Shape
Multiple diverticula



Megacalyces
Other Ureteral Abnormalities
Hematuria
Ureteral Notchingsecondary to retroperitoneal varices fromhighly vascular renal cell carcinoma

Causes of Ureteral Notching
Arterial: renal/iliac/aortic aneurysm
Venous: normal or enlarged gonadal veins, rightovarian vein syndrome, varicocele and varices ofbroad ligament, occlusion IVC below renal veins bytumor, RPF, clot, surgery; occlusion IVC aboverenal veins by thrombus or tumor; occlusion SVCby tumor, portal hypertension
Kawashima, etal. Radiographics 2000;20,1321

Urinary Tract Tuberculosis
Neo-ureter

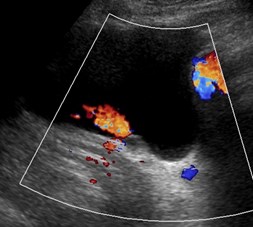
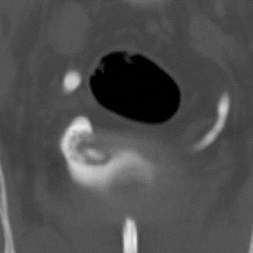
39 year old woman with historyof breast cancer

Sagittal R adnexa
Pelvic endometriosiscausing bilateralhydroureteronephrosis
Deep Endometriosis
Defined as endometriosis penetratingretroperitoneal space or wall of pelvicorgans to at least 5mm
involves retroperitoneum and recto-vaginal septum> vagina> bowel>bladder> ureter
Causes significant pain, urinary andbowel symptoms and infertility
Deep Endometriosis
Histology: fibromuscular hyperplasiasurrounds foci of endometriosis infiltratingadjacent tissues, forming solid nodules
Involvement of ureter causes hydroureter andhydronephrosis, often isidious onset
Usually extrinsic involvement of distal 1/3 ofureter, occasionally invasive
Bladder involvement more common, usually as2-4 cm mass in dome with other disease
Bazet. Radiology 2004;232:379
Del Frate. Radiographics 2006;26:1705

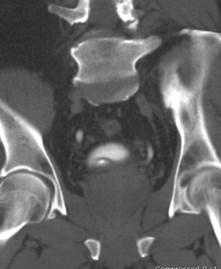
69 year old with history of prostate carcinoma
Benign Ureteral Stricture
Causes: surgery, trauma, radiationtherapy, infection, calculous disease,retroperitoneal fibrosis
73 year old



Retroperitoneal Fibrosis
Inflammatory aneurysm causing medial deviation of ureters

Hematuria in 68 year old
Retroperitoneal Fibrosis
Typically peri-aortic distribution
May encase ureters, extend into renalhilum.
Localized peri-ureteral fibrosis may bedue to chronic indwelling ureteralstent, sarcoidosis, malignancy
62 year old man





7-6-06
Retroperitoneal fibrosis secondary to inflammatory aneurysm
Treated with vascular and ureteral stents


Two different patients
Pseudodiverticulosis
Definition: < 5mm sized out pouchingsof hyperplastic transitional epitheliuminto subepithelial connective tissuewith associated chronic inflammatorychanges
Do not penetrate muscular wall and areNOT true diverticula
Pseudodiverticulosis
First described in 1957
Associated with chronic urinary tract infections
Significant association with urothelialmalignancy
Post mortem study of 200 ureters showed 11%incidence often with associated microscopicureteritis cystica and glandularis but noassociated malignancy
Wasserman AJR 1991;157:69


Pyeloureteritis Cystica
2 – 3 mm sized smooth filling defects
Multiple small, subepithelial fluid filledcysts in wall with inflammatory changes
Cystic foci of glandular metaplasia
Not malignant, controversial if pre-malignant.
Differential diagnosis: multiple TCCs,bubbles, calculi, vascular impressions
Kawashima Radiographics 2004;4:535
Figure 11b. Ureteritis cystica of the left ureter in a 60-year-oldwoman with a history of left renal stone
Kawashima A et al. Radiographics2004;24:S35-S54
©2004 by Radiological Society of North America
http://www.imagingsciencetoday.com/teaching-case/gu-radiology/20090608/ureteritis-cystica-radiologic-pathologic-correlation-256.html
Mt. Ranier, WA, June 2008